Our Patients:
Quincy Rainey

Before February 2026, Quincy was a healthy, highly active 17‑year‑old junior at Rockwood Summit High School. A dedicated multi-sport athlete, he trained year-round and was accustomed to intense physical demands, pushing through injuries and conditioning seven days a week. Quincy was being scouted by colleges for athletic scholarships and maintained a full academic and extracurricular schedule. Outside of athletics, he was actively involved in Fellowship of Christian Athletes and Campus Ministry and took great pride in being a big brother to his siblings, Melanie (9) and Daniel (7).
“Quincy has always been driven,” his mother, Michelle, said. “He’s up early for workouts, stays late with his teammates, and still makes time for his studies, family and friends. Being active is just who he is.”
Aside from a brief period of intermittent illness—low-grade fever and what was believed to be bronchitis—there were no warning signs that Quincy was facing a serious condition. He was participating in sports and all of his normal daily activities, until a sudden episode of dizziness at school raised concern.
“The school nurse called me when Quincy got dizzy walking up the stairs,” Michelle recalled. “That was totally unlike him, so we went straight to his pediatrician that afternoon.”
Out of concern for possible pneumonia, the pediatrician referred the family to the Emergency Department at SSM Health Cardinal Glennon Children’s Hospital. Instead, Quincy was diagnosed with compensated heart failure, with impaired function affecting one side of his heart.
“I kept saying, ‘Tell me again what you said,’” Michelle said. “Heart failure just didn’t make sense. He had been running the day before.”
Quincy was admitted to the Pediatric Intensive Care Unit (PICU) that afternoon, on February 4, 2026, and started on intravenous medications to support his cardiac function. A comprehensive diagnostic workup began, including genetic and viral testing, to identify the underlying cause of his heart failure and guide long-term treatment. “At that point, all we knew was that we would be there for at least several days while they figured out a cause and an action plan,” Michelle said.
The cardiology team initially aimed to transition Quincy from IV to oral heart medications with close inpatient monitoring. His heart was enlarged with a gallop rhythm and his BNP (B‑type natriuretic peptide) levels—used to assess heart failure severity—were higher than normal. (For reference, BNP levels below 100 pg/mL are considered normal.)
Despite early signs of stabilization, Quincy’s clinical status deteriorated. His BNP levels rose significantly, reaching 7,500 pg/mL (up from 5,500 pg/mL on admission), and his oxygen levels declined. “It seemed like his body got sicker overnight,” Michelle said.
Given the progression of heart failure, Quincy was restarted on IV medications and evaluated for heart transplantation. Over the next one to two weeks, he underwent extensive laboratory testing, imaging, and multidisciplinary consultations to ensure his body could tolerate transplant surgery.
A cardiac catheterization performed on February 25 unexpectedly revealed elevated pulmonary vascular resistance and high intracardiac pressures, making the possibility of transplant unsafe. “The doctors explained that if he had received a heart at that point, his body would have rejected it,” Michelle said. “He needed something immediately to keep him stable and hopefully get him to transplant later on.”
The very next day, on February 26, Quincy underwent open-heart surgery for placement of a Left Ventricular Assist Device (LVAD) to support cardiac output and lower pulmonary pressures. And the next day, a temporary Impella device was placed to relieve pressure on the right side of his heart.
Despite the complexity of his condition, Quincy demonstrated amazing resilience post-operatively. He was extubated on March 1, had the Impella removed on March 4, and walked a full lap around the PICU by March 5. “They told us over and over, ‘Quincy is made of steel,’” Michelle shared.
Over the following weeks, Quincy’s care focused on optimizing LVAD settings, transitioning to oral medications, and building strength through physical and occupational therapy. By mid-March, he was discharged home with close outpatient monitoring. “It was the greatest gift ever to be able to go home,” said Michelle. It was definitely what our whole family needed, and we just took everything day by day.”
A repeat cardiac catheterization on March 30 showed improved hemodynamics, allowing Quincy to be officially placed on the heart transplant list in early April. He was listed as Status 1A, the highest priority for heart transplantation.
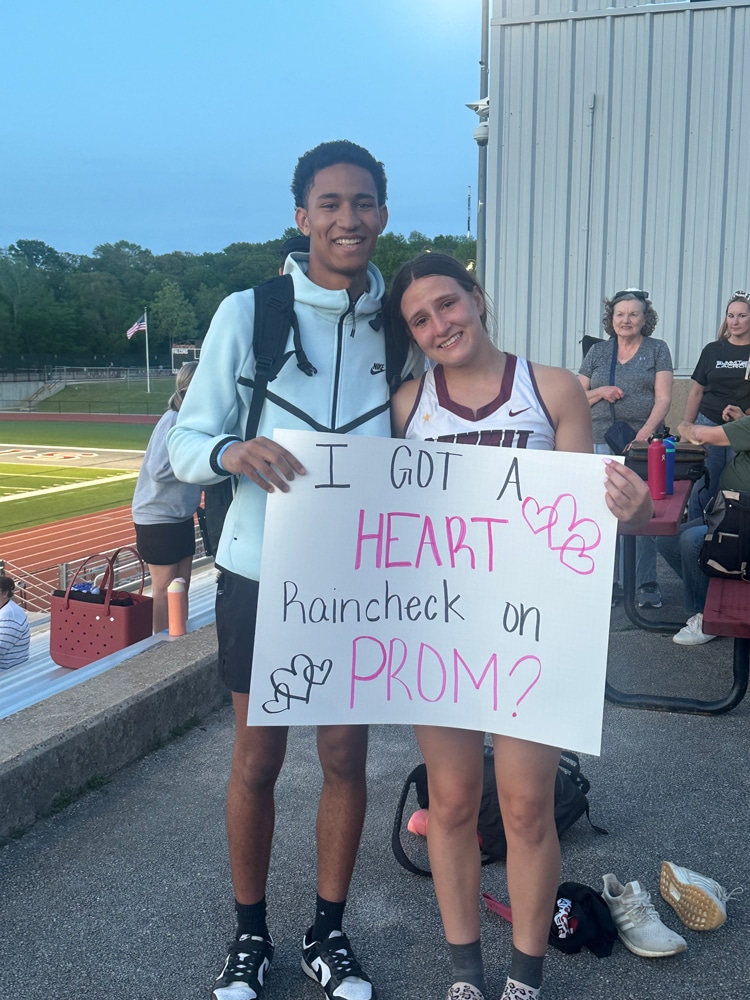
On April 23 at 5:04 p.m., the family received the call that a donor heart was available. The timing was especially memorable since April is Organ Donation Awareness Month and because Quincy’s junior prom was scheduled for April 24. “He told his girlfriend he had to have a raincheck to prom because he had a date with a new heart,” Michelle said. On April 24, Quincy underwent heart transplant surgery, which lasted approximately 11.5 hours. In proper celebratory spirit, his girlfriend came to the hospital the next day to be right by his side—wearing her prom dress.
Quincy was extubated on April 27 and resumed walking laps around the PICU by April 30. His postoperative recovery involved careful management of medications, fluid status, and gradual strengthening.
“The team explained that his body had been functioning on about 20% heart capacity,” Michelle said. “It was incredible what he was able to do before—and now he has a healthy heart.
Just two weeks after transplant, on May 8, Quincy was discharged home.
“There are no words big enough to express our gratitude,” Michelle said. “A donor family chose to say yes, and because of them, Quincy gets to keep living his life. We think about them constantly and will honor them every day.”